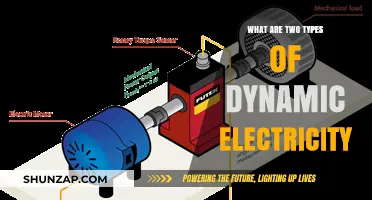
Defibrillation is a critical intervention for treating life-threatening cardiac arrhythmias, specifically ventricular fibrillation and pulseless ventricular tachycardia. It involves delivering a controlled electrical shock to the heart, allowing it to return to a normal rhythm. When a patient's heart is in ventricular fibrillation or ventricular tachycardia, the electrical signals that control the heart are scrambled, resulting in a chaotic and ineffective rhythm. Defibrillation provides a sudden burst of energy through the patient's heart, causing their heart cells to depolarize and stop the abnormal rhythm. This process is known as defibrillation and can be life-saving in cases of sudden cardiac arrest.
| Characteristics | Values |
|---|---|
| Treatment | Electrical defibrillation |
| Purpose | To depolarize the heart muscle and allow the sinoatrial node to reestablish a coordinated rhythm |
| Indication | Cardiac arrest with ventricular fibrillation (VF) or pulseless ventricular tachycardia (VT) |
| Effectiveness | Most effective when performed immediately after onset; success rate declines by ~10% for each minute of delay |
| Availability | Widespread availability of automated external defibrillators (AEDs) allows trained first responders and laypersons to provide early defibrillation |
| Limitations | Not indicated if the patient is conscious or has a pulse; improper shocks can cause dangerous dysrhythmias |
Explore related products






What You'll Learn
![]()
Ventricular fibrillation (VF)
In a typical heart, electrical signals travel from the upper chambers (atria) to the lower chambers (ventricles), causing the ventricles to contract and pump blood. However, in ventricular fibrillation, rapid and irregular electrical signals cause the lower chambers to quiver uselessly instead of pumping blood. This is known as "quivering of the heart muscle". As a result, the heart abruptly stops pumping blood to the body, causing a sudden drop in blood pressure. If left untreated, ventricular fibrillation can lead to death within minutes as the vital organs, including the brain and spinal cord, are starved of oxygen.
Ventricular fibrillation most commonly occurs within diseased hearts and is often a manifestation of underlying ischemic heart disease. It is also associated with cardiomyopathy, myocarditis, and other heart pathologies, as well as electrolyte imbalance, drug overdoses, near drowning, and major trauma. In some cases, ventricular fibrillation occurs with no discernible heart pathology or other evident cause, known as idiopathic ventricular fibrillation.
The definitive treatment for VF is electrical defibrillation, which is most effective when performed immediately after the onset of VF. For each minute of delay, the success rate of defibrillation declines by about 10%, and after 10 minutes, the chances of successful resuscitation drop to near zero. Cardiopulmonary resuscitation (CPR) can be performed until defibrillation is possible, and medications such as epinephrine or amiodarone may be given if defibrillation is unsuccessful.
BDO's Power Waste: Idle Trays Costing the Earth?
You may want to see also
Explore related products






![]()
Pulseless ventricular tachycardia (VT)
People experiencing pulseless VT are unconscious and unresponsive, with no palpable pulse. Before becoming unconscious, they may exhibit symptoms such as chest pain, heart palpitations, lightheadedness, shortness of breath, and a decreased level of consciousness.
The diagnosis of pulseless VT is based on physical examination and electrocardiogram (ECG) findings. ECG criteria for diagnosing VT include regular R-R intervals, a rapid ventricular rate with an undistinguishable atrial rate (absence of p-waves), AV dissociation, and a wide QRS complex.
The treatment for pulseless VT follows Advanced Cardiac Life Support (ACLS) guidelines, which include high-energy unsynchronized defibrillation at 360J for a monophasic defibrillator or 200J for a biphasic defibrillator. Cardiopulmonary resuscitation (CPR) should be initiated immediately upon confirmation of the diagnosis, and epinephrine and other antiarrhythmic drugs may be administered to help terminate the rhythm.
The prognosis for pulseless VT heavily depends on the time from the onset of tachycardia to defibrillation and the restoration of sinus rhythm. Shorter delays in defibrillation are associated with higher survival rates, while delays in treatment of more than 15 minutes can decrease survival rates to as low as 5%.
To prevent recurrence of VT, long-term anti-arrhythmic therapy may be indicated, including beta-blockers and class III anti-arrhythmic drugs. An implantable cardioverter defibrillator (ICD) is also an effective option for preventing sudden cardiac death due to VT, although it does not prevent the occurrence of VT or VF.
Shaving Armpits: Electric Razor Techniques for Smooth Results
You may want to see also
Explore related products





![]()
Supraventricular tachycardia (SVT)
While some patients with SVT may exhibit few or no symptoms, others may experience severe signs and symptoms related to the rapid heart rate, including chest pain, respiratory distress, hypotension, altered mental status, or dizziness. It is crucial to differentiate SVT from ventricular tachycardia, as their management strategies differ. To diagnose SVT, healthcare professionals use an electrocardiogram (ECG) to identify the characteristic narrow complex and confirm the presence of tachycardia.
The treatment for SVT aims to restore a normal heart rhythm and prevent recurrence. Initial treatment options include vagal maneuvers, such as applying pressure to specific areas of the neck (carotid sinus massage) or having the patient lie down in the supine position. If these measures are ineffective or the patient is unstable, synchronized electrical cardioversion may be necessary. This procedure involves delivering a precisely timed shock during the "R" wave on the EKG to avoid the vulnerable refractory period, which could lead to ventricular fibrillation. The shock voltage for cardioversion in adults is typically between 50 and 100 J, while lower doses are used for children.
In certain cases, catheter ablation may be considered to eliminate the areas causing abnormal electrical signals. This procedure has a high cure rate, surpassing 95% depending on the SVT type. Additionally, pharmacotherapy may be used to manage SVT, but it is important to be cautious of potential side effects. Patients with recurrent SVT should receive coordinated follow-up care, including timely access to specialty care and continuous monitoring of treatment efficacy and adverse effects.
Electric Scooters: How Fast Can They Go?
You may want to see also
Explore related products




![]()
Wolff-Parkinson-White syndrome
Wolff-Parkinson-White (WPW) syndrome is a rare congenital heart abnormality that affects 1 to 3 people per 1,000 worldwide. It is characterised by an abnormal electrical condition in the heart, resulting in a rapid heart rate or tachycardia. The condition was first described in 1915 by Frank Norman Wilson, and later in 1930 by cardiologists Louis Wolff, John Parkinson, and Paul Dudley White, who identified a distinct electrocardiograph (ECG) pattern in healthy young people with short bursts of rapid heart rate.
WPW syndrome is caused by an extra piece of heart muscle that creates an additional electrical conduction pathway, known as an accessory pathway, between the heart's upper and lower chambers. This extra pathway disrupts the normal coordinated movement of electrical signals, causing the heart to beat faster than usual. The condition can lead to periods of rapid heart rate, with some individuals experiencing heart rates of over 100 beats per minute. The fast heart rate, or tachycardia, can come and go suddenly and may result in severe hypotension and syncope, or loss of consciousness.
The condition is typically diagnosed by a physician through a thorough clinical evaluation, detailed patient history, and specialised tests such as an electrocardiogram (EKG), electrophysiologic studies (EPS), and Holter Monitor testing. Treatment for WPW syndrome depends on the severity and frequency of symptoms. Some treatments aim to stop episodes of fast heartbeats, while others focus on preventing future episodes. Vagal maneuvers, such as coughing or "bearing down," can help stimulate the vagus nerve to control the heartbeat. Pharmacological treatments can also be prescribed to slow or regulate the heartbeat. Radiofrequency ablation is a procedure with a high success rate that involves sending energy to the area of the heart with an electrical problem, causing scarring and allowing the heart to beat normally. Cardioversion, which involves giving the heart an electrical shock to stop the fast heartbeat, may also be considered.
While most people with WPW syndrome do not have any other heart problems, the condition has been associated with other cardiac conditions such as Ebstein's anomaly, a congenital heart defect affecting the tricuspid valve. WPW syndrome carries a small risk of sudden death, which may be due to rapidly conducted atrial fibrillation causing ventricular fibrillation. However, the overall risk is approximately 2.4 per 1,000 person-years, and the condition is successfully treated in many cases.
Repairing Your Fridge: Fixing a Damaged Electric Cord
You may want to see also
Explore related products





![]()
Long QT syndrome
LQTS can be inherited, meaning you are born with the condition, or acquired, meaning you develop it during your lifetime. It is often a lifelong condition, and while the risk of abnormal heart rhythm may lessen with age, it never completely disappears. LQTS is caused by ion channels on the surface of heart muscle cells not functioning properly or being insufficient in number. These ion channels regulate the flow of electrically charged sodium, calcium, and potassium atoms, and their dysfunction can disrupt the electrical activity in the heart's lower chambers or ventricles, leading to dangerous arrhythmias.
The diagnosis of LQTS involves taking a detailed medical and family history, reviewing symptoms, and assessing medications. Physical examinations and various tests, such as blood tests, genetic testing, EKGs, and stress tests, are also employed to confirm the condition. Treatment focuses on preventing arrhythmias and fainting spells, but it does not cure the disorder or necessarily restore a normal QT interval. For those with acquired LQTS, addressing the underlying conditions or discontinuing certain medications can resolve the issue.
LQTS can lead to sudden uncontrollable fast heart rhythms, which, if they result in cardiac arrest, may be treated with defibrillation. Defibrillation is a critical intervention that uses a controlled electrical shock to depolarize the heart muscle, allowing it to reestablish a coordinated rhythm. Early defibrillation is crucial, as survival rates decrease with each minute of delay, and the chances of successful resuscitation drop significantly after 10 minutes.
Electricity Basics: Lighting a Bulb
You may want to see also
Frequently asked questions
Defibrillation is a critical intervention for treating life-threatening cardiac arrhythmias, specifically ventricular fibrillation and pulseless ventricular tachycardia. It uses an electrical charge to stop the heart's abnormal rhythm and allow it to start a normal rhythm again.
Electrical defibrillation is indicated when a patient experiences cardiac arrest due to ventricular fibrillation or pulseless ventricular tachycardia. It is most effective when performed immediately after the onset of ventricular fibrillation.
There are internal and external defibrillators. External defibrillators can be manual or automated (AED). AEDs are designed to be used by untrained or briefly trained laypersons and provide step-by-step voice instructions to guide the user.
The success rate of defibrillation declines by about 10% for each minute of delay, and after 10 minutes of ventricular fibrillation, the chances of successful resuscitation drop to near 0%. However, early defibrillation within the first 3 to 5 minutes of arrest can dramatically improve survival outcomes.